Cannabis
Why the High Isn’t Worth it if Pregnant or Breastfeeding
Disclaimer: This page houses important information and resources pertaining to cannabis in pregnancy and while breastfeeding, including links to our evidence-based Fact Sheets. However, the resources here should not replace the care and advice of a medical professional.
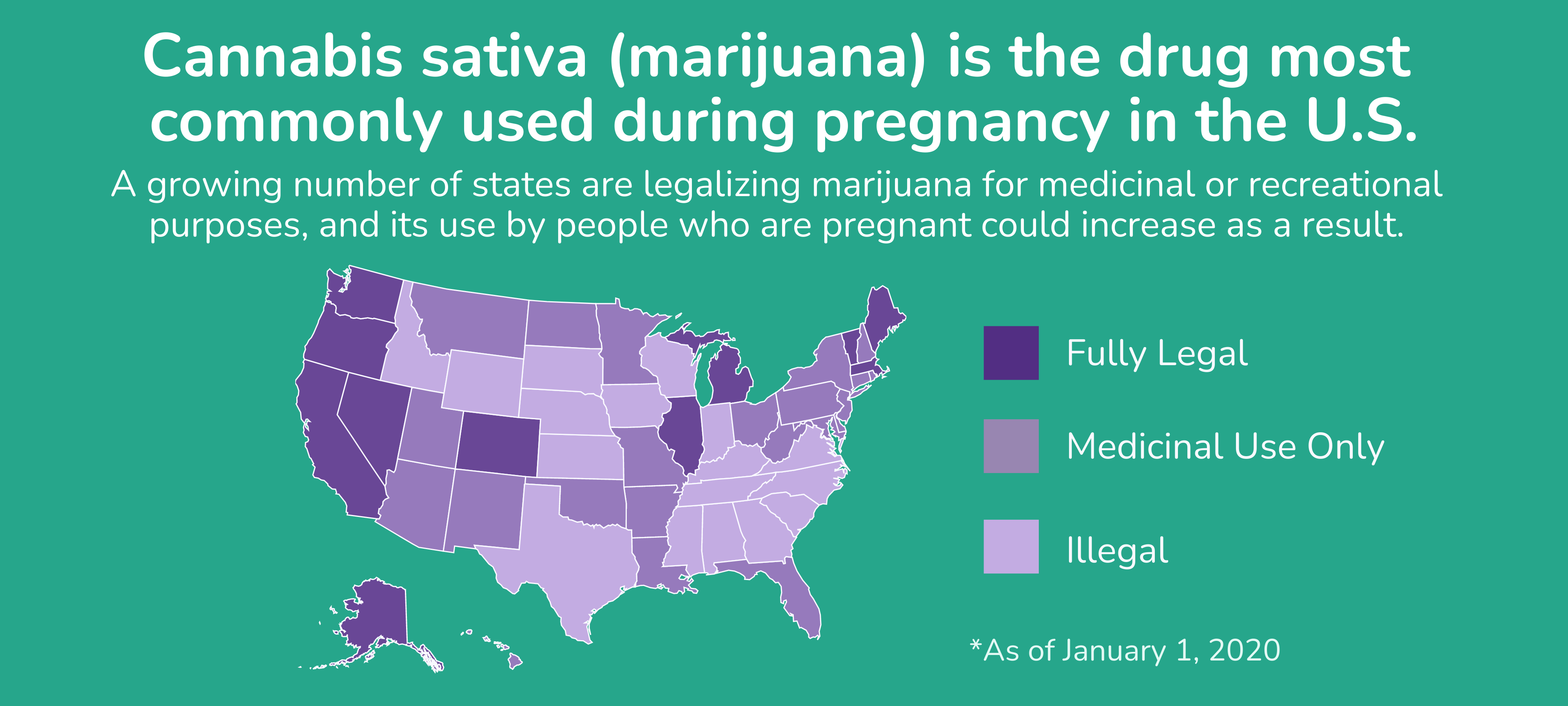
Many moms may not want to hear this, but medical experts agree: cannabis (commonly known as marijuana, weed, or pot, among many other terms) should be avoided if you are pregnant or breastfeeding. Cannabis use during pregnancy has been linked to an increased risk for some pregnancy complications, such as preterm birth and having a low birth weight baby. Babies that are born prematurely or with low birth weight can have higher rates of learning problems or other disabilities. In addition, chemicals in cannabis (in particular, tetrahydrocannabinol or THC, which is the primary component of marijuana that produces a “high”) cross the placenta and reach the baby, and there is some concern that this exposure could cause long-term learning or behavior problems.
“When cannabis (marijuana) is smoked or eaten, the chemicals reach the fetus by crossing the placenta. Research is limited on the harms of marijuana use during pregnancy. But there are possible risks of marijuana use, including babies that are smaller at birth and stillbirth. The American College of Obstetricians and Gynecologists recommends that pregnant women not use marijuana.”
— American College of Obstetricians and Gynecologists Committee Opinion No. 722
THC can also be passed to a baby through breast milk. THC is stored in fat and is slowly released over time, meaning a baby could still be exposed even after mom stops using cannabis. A study led by our own Dr. Christina Chambers found that THC may be present in a mom’s breast milk up to 6 days after last use. Because a baby’s brain continues to develop during the time that they are being breastfed, experts worry about the possible effects this exposure may have on a nursing infant when a mother uses cannabis during breastfeeding.
Reference: American College of Obstetricians and Gynecologists (ACOG) and Business Insider
Please see our library of resources below on cannabis exposure during pregnancy and breastfeeding.
External Resources
- March of Dimes: Pregnancy and Marijuana Use
- Substance Abuse and Mental Health Services Administration (SAMHSA): Marijuana and Pregnancy
- U.S. Centers for Disease Control and Prevention (CDC): Breastfeeding and Marijuana
- U.S. Centers for Disease Control and Prevention (CDC): What You Need To Know About Marijuana Use and Pregnancy
- U.S. Food and Drug Administration (FDA): What You Should Know About Using Cannabis, Including CBD, When Pregnancy or Breastfeeding