MotherToBaby Interactive Critical Periods of Pregnancy Tool
Understanding Critical Periods in Pregnancy
Kendra, newly pregnant at approximately 7 weeks along, contacted MotherToBaby late one afternoon with a question that had been causing her a lot of anxiety. Norovirus was running rampant in her home, and she was feeling extremely nauseous. Having found relief with it before, she explained that she had taken a single dose of Zofran (ondansetron) early that morning. She was certain this drug was ok to take during pregnancy, but after searching online, she became concerned. Kendra shared that she had read conflicting information about whether Zofran increased the risks for birth defects; with some studies showing an increased chance of heart defect and cleft palate, and other studies showing no increased risk. Feeling confused, Kendra reached out to MotherToBaby with her question to receive personalized information.
On the call, I first explained that birth defects can happen in any pregnancy for different reasons. Out of all babies born each year, about 3 out of 100 (3%) will have a birth defect. Pregnancy problems (like miscarriage) can also happen in any pregnancy. Sometimes, exposures like medications, drugs, alcohol, and infections can increase the chance for birth defects or pregnancy complications. However, for an exposure to cause a problem, it generally has to happen during the “critical period” when a body part is forming.
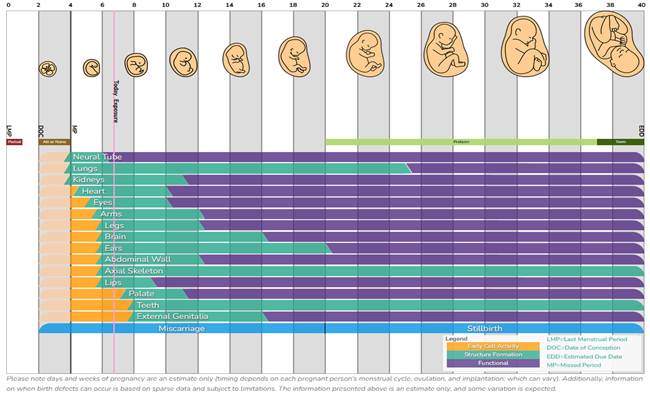
To help Kendra understand more about possible risk from her Zofran exposure, I used MotherToBaby’s new and interactive critical periods of pregnancy tool! This helpful pregnancy calculator and chart shows when different parts of a baby’s body form during pregnancy and when birth defects or pregnancy complications might happen. By entering the first day of your last menstrual period (LMP) or estimated due date (EDD), the calculator can estimate how far along you are today. Individuals who have questions about exposures in pregnancy can then go on to enter the specific date(s) when the exposure (such as medication use or alcohol consumption) occurred, and the chart will show the body parts that are developing during that time.
After entering the first day of Kendra’s last period, the interactive tool confirmed she was 6 weeks and 5 days pregnant. I then entered her Zofran exposure using today’s date, which resulted in a pink line popping up on the chart. Following this line down the chart, I could see all of the different body parts that were currently forming. I explained to Kendra that when she took the Zofran, the palate (roof of the mouth) had not yet started to form, meaning that the medication use was unlikely to increase the chance of cleft palate in the baby. The chart also helped me see that the baby’s heart was currently developing. I shared this with Kendra, but also reminded her that the latest research shows there is thought to be a less than 1% chance of heart defects from exposure to Zofran; meaning there is a more than 99% chance the heart will not be affected by her medication use. In other words, even when an exposure of concern takes place during the critical period, not every baby will be affected by that birth defect.
For Kendra, being able to understand which specific body parts were forming when she took the Zofran and whether she actually needed to be concerned helped decrease her anxiety significantly. Knowing that the heart was currently forming, she decided to reach out to her healthcare provider to discuss alternative treatment options for her nausea. I was happy to have helped answer Kendra’s question using this visual tool and look forward to being able to use it again in the future when pregnant women have questions about the timing of their exposure.
Remember that our team is always available to help review any exposures you have had and provide a personalized risk assessment. Don’t hesitate to contact MotherToBaby by phone, chat, text, or email!

