Cannabis
This sheet is about exposure to marijuana in pregnancy and while breastfeeding. This information is based on published research studies. It should not take the place of medical care and advice from your healthcare provider.
What is marijuana?
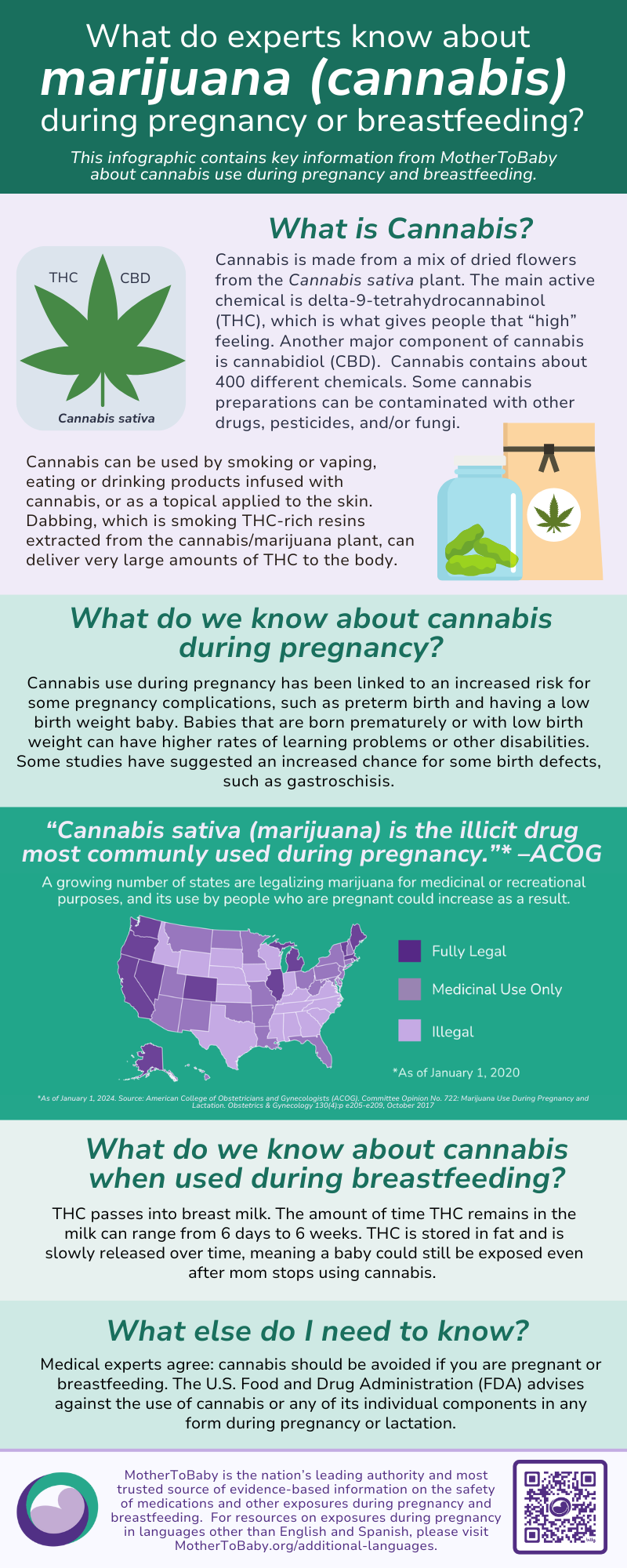
Marijuana is a mix of dried leaves, seeds, stems, and flowers from the Cannabis sativa or Cannabis indica plant. Some other names for marijuana are pot, weed, and cannabis. The main active chemical in marijuana is delta-9-tetrahydrocannabinol (THC), which is what gives a “high” feeling. Some of the ways people use marijuana or THC include smoking or vaping (inhalation), eating or drinking products (ingestion) that contain marijuana or THC (edibles), and applying products that contain marijuana or THC to the skin (topical use).
In addition to THC, another active chemical in marijuana is cannabidiol (CBD). CBD is sold in many kinds of products, such as coffees, chocolates, supplements, tinctures, cosmetics, lotions, suppositories, and bath salts. CBD products labeled as “THC free” might still contain a measurable amount of THC.
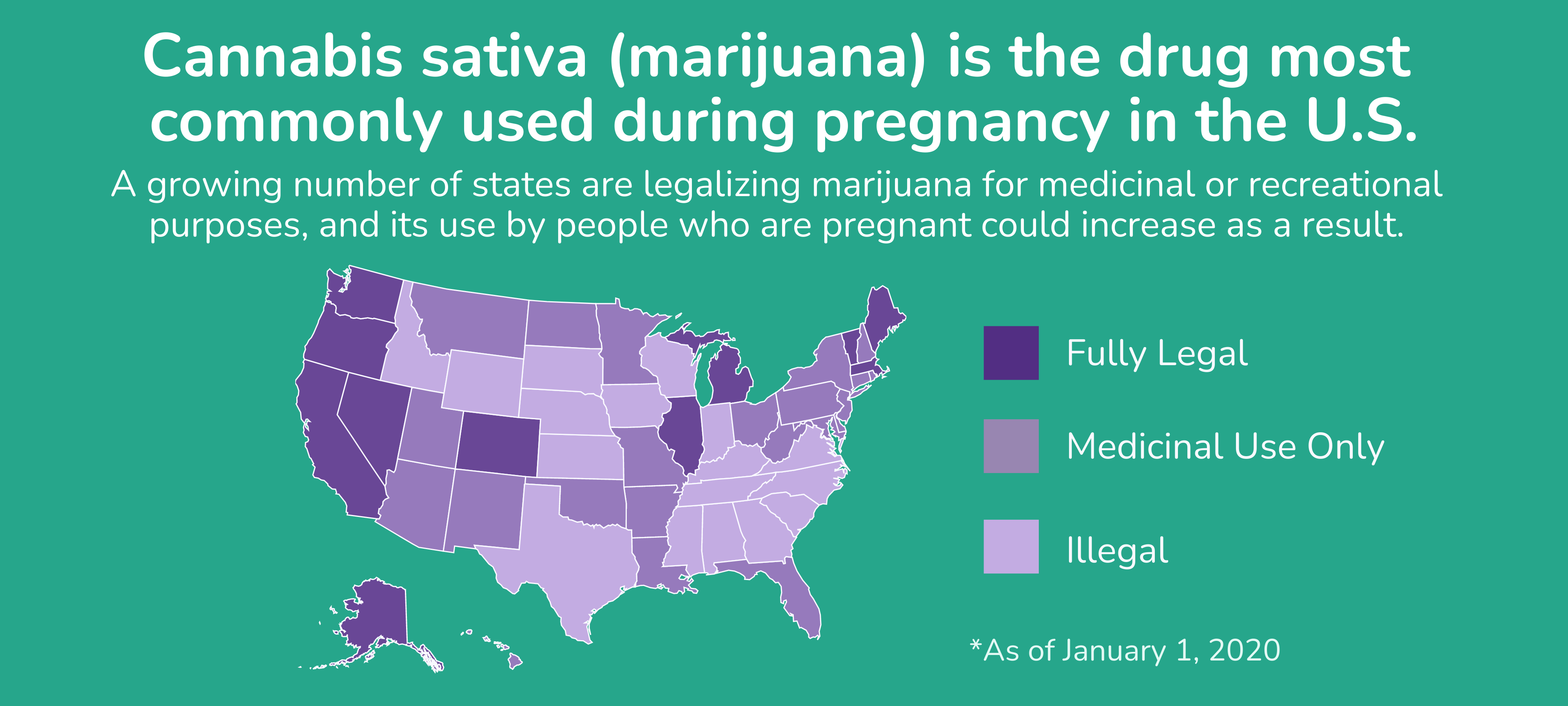
The American Academy of Pediatrics (AAP) recommends that women who are pregnant or breastfeeding avoid using marijuana. The American College of Obstetricians and Gynecologists (ACOG) advises that women who are planning pregnancy, currently pregnant, or breastfeeding avoid using marijuana. The U.S. Food and Drug Administration (FDA) advises against using CBD, THC, and marijuana in any form during pregnancy or while breastfeeding.
I use marijuana, but I would like to stop before getting pregnant. How long does the drug stay in my body?
The time it takes the body to metabolize (to process) drugs is not the same for everyone. In healthy non-pregnant adults, it takes up to 14 days, on average, for most of the THC to be gone from the body. However, the way marijuana is used (inhaled, ingested, used topically), how often it is used, and how much is used can affect how long the THC and other active chemicals in marijuana stay in the body.
I use marijuana. Can it make it harder for me to get pregnant?
It is not known if marijuana can make it harder to get pregnant. Some studies suggest that regular use of marijuana might affect the menstrual cycle (a woman’s period or ovulation (release of an egg from the ovaries)), which could make it harder to get pregnant.
Does using marijuana increase the chance of miscarriage?
Miscarriage is common and can occur in any pregnancy for many different reasons. It is not known if using marijuana can increase the chance of miscarriage. One study found a higher chance of miscarriage among women who used marijuana. Other studies have not found a higher chance of miscarriage.
Does using marijuana increase the chance of birth defects?
Birth defects can happen in any pregnancy for different reasons. Out of all babies born each year, about 3 out of 100 (3%) will have a birth defect. We look at research studies to try to understand if an exposure, like marijuana, might increase the chance of birth defects in a pregnancy.
Some studies have suggested that using marijuana during pregnancy increases the chance of birth defects, including heart defects, genital defects, defects of the central nervous system (CNS) (brain and spinal cord), and intestinal defects such as gastroschisis (a hole in the belly wall where the intestines can poke out through the skin). Other studies have not found a higher chance of birth defects in pregnancies exposed to marijuana. It is difficult for researchers to confirm how much and how often a person uses marijuana in pregnancy, and how much THC or other chemicals they are exposed to in the products they use, or if they are also using other substances. These limitations make it hard to know if marijuana can increase the chance of birth defects.
Does using marijuana in pregnancy increase the chance of other pregnancy-related problems?
Some studies have suggested a higher chance of pregnancy-related problems such as preterm delivery (birth before week 37), low birth weight (weighing less than 5 pounds, 8 ounces [2500 grams] at birth), small length, small head size, and stillbirth among women who smoke marijuana regularly. Some of these studies suggest that the more a woman uses marijuana during pregnancy, the higher the chance of these complications. The difficulties with studying marijuana use during pregnancy make it hard to know if these complications are caused by the marijuana use, the use of other substances that can increase these risks (such as cigarettes), or other factors.
Some studies have suggested that prenatal use of marijuana increases the chance of health problems for the woman during pregnancy such as high blood pressure, problems with the placenta, and effects on pregnancy weight gain. The studies were not able to look at some other important factors that could have increased the chances of these outcomes, such as problems in previous pregnancies, other underlying health conditions, and the use of some other substances. This makes it hard to know if the marijuana, other factors, or a combination of factors might be the cause of these pregnancy problems.
If I use marijuana throughout my entire pregnancy, will it cause withdrawal symptoms in my baby after birth?
There are reports of temporary symptoms, such as jitteriness and irritability, in newborns who were exposed to marijuana during pregnancy. There are also reports of babies who did not have these symptoms. It is important that your healthcare providers know if you are using marijuana so that if symptoms occur your baby can get the care that is best for them.
Does using marijuana in pregnancy affect future behavior or learning for the child?
Studies have shown that prenatal exposure to marijuana can change how the brain develops, but it is not clear if or how these changes affect learning or behavior later in life. Some studies of children and/or adolescents who were exposed to marijuana during pregnancy report more problems with executive function (such as the ability to plan, focus, remember, and multi-task) and problems doing well in school. In some studies, exposed children and/or adolescents are reported to have more impulsive, hyperactive, aggressive, or disruptive behavior and/or to be more likely to experience depression, anxiety, and substance use. Some of these issues have been reported more often in children of “heavy” marijuana users (users who reported smoking one or more marijuana cigarettes per day) than in children of less frequent marijuana users. The difficulties with studying marijuana use during pregnancy make it hard to know if these issues in children and adolescents are caused by the marijuana use, other factors, or a combination of factors. Other studies have not found increased behavior or learning issues in children or adolescents with prenatal exposure to marijuana.
What screenings or tests are available to see if my pregnancy has birth defects or other issues?
Prenatal ultrasounds can be used to screen for some birth defects, such as defects of the heart, genitals, CNS, and intestines. Ultrasound can also be used to watch the growth of the pregnancy. Talk with your healthcare provider about any prenatal screenings or testing that are available to you. There are no tests available during pregnancy that can tell how much effect there could be on future behavior or learning.
Breastfeeding while using marijuana:
THC passes into breastmilk. The amount of time THC stays in the milk can range from 6 days to 6 weeks. Some studies on the use of marijuana in breastfeeding suggest a delay in motor development (learning to crawl and walk on time) in the child. Other studies have not proven clear health concerns for a child exposed to marijuana through breast milk.
Use of marijuana might affect levels of prolactin (a hormone that helps the body make milk). Low prolactin levels could reduce the amount of milk produced. Using marijuana might also change the quality of breast milk, including the amounts of nutrients such as fat and protein.
Professional organizations including AAP, ACOG, and FDA advise that women who are breastfeeding avoid using marijuana. Be sure to talk to your healthcare provider about all your breastfeeding questions.
If a man uses marijuana, could it affect fertility or increase the chance of birth defects?
Marijuana use can affect the number, size, shape, and movement of sperm. These changes in the sperm might affect a man’s fertility (ability to get a woman pregnant). In general, exposures that fathers or sperm donors have are unlikely to increase risks to a pregnancy. For more information, please see the MotherToBaby fact sheet Paternal Exposures at https://mothertobaby.org/fact-sheets/paternal-exposures-pregnancy/.
Please click here for references.